d-Transposition of the Great Arteries
Quick Facts
- In d-transposition of the great arteries, the heart’s main arteries are connected to the wrong chambers (switched positions).
- When a baby is born with d-TGA, treatment is needed quickly to ensure survival.
- Children and adults who have had d-TGA surgery need regular care from a specialist in congenital heart disease.

What is d-transposition of the great arteries?
In this condition, the heart’s two main arteries are switched.
Normally, blood follows this path: body → heart → lungs → heart → body.
With d-transposition, the arteries are connected to the wrong chambers of the heart. This changes the normal flow of blood. Instead of moving through the lungs to pick up oxygen and then going to the body, the blood circulates in separate loops:
- Body → heart → body, without going to the lungs for oxygen
- Lungs → heart → lungs, without carrying oxygen to the body
As a result, the body does not get enough oxygen. Without surgery or adequate mixing of blood, babies can survive for only a short time. Before surgery, natural or medically created openings in the heart may allow some oxygen-rich blood to mix with oxygen-poor blood.
This condition is usually more severe early in life than L-transposition of the great arteries. In d-TGA, blood circulates in separate loops, and the body does not get enough oxygen. In L-TGA, the heart’s structure allows blood to flow in a more normal pattern, so symptoms may be milder at first.
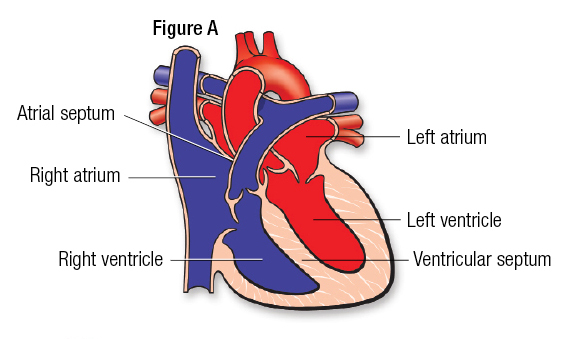
The heart has four chambers. The upper two chambers are the atria, and the lower two are the ventricles (Figure A). The chambers are separated by a wall of tissue called the septum. Blood is pumped through the chambers, aided by four heart valves. The valves open and close to let the blood flow in only one direction.
What causes d-transposition?
The cause is unknown, but genetic factors may contribute to it. Uncontrolled diabetes during pregnancy is associated with a higher risk of d-TGA.
How is d-transposition treated?
Babies born with d-transposition of the great arteries need surgery early in life to survive.
Before surgery, many infants have a temporary procedure done in a cardiac catheterization lab. This procedure helps stabilize the baby until they are strong enough for surgery. It enlarges a natural opening between the right and left upper chambers (the atria), a procedure called balloon atrial septostomy. This lets oxygen-rich blood mix with oxygen-poor blood, delivering more oxygen to the body.
The most common surgery used is an arterial switch operation. The two main arteries are moved to their normal positions. The aorta is connected to the left side of the heart, and the pulmonary artery is connected to the right side. The coronary arteries, which supply blood to the heart muscle, are also reattached.


d-Transposition in children: What families need to know
What type of problems might my child have?
Children who have had the arterial switch operation may have valve leakage, narrowing of the great arteries, or coronary artery problems.
Will my child need more surgery?
Children who had the arterial switch operation may need more surgery to relieve narrowing in the aorta or pulmonary artery where the original surgery was done or to fix leaky valves.
Will my child’s activities be limited?
Many children with d-TGA can be active. In general, health care professionals encourage physical activity because it supports heart health, fitness and overall well-being. Talk with your child’s cardiologist about sports and more intense activity to help determine if limitations are needed.
What will my child need in the future?
Children with d-transposition will need lifelong care from an adult congenital heart specialist. Some may need medications to help the heart work as well as possible.
Regular checkups are important so the cardiologist can monitor heart health over time. To do this, your child may have routine, non-invasive tests. These can include electrocardiograms, Holter monitors, exercise stress tests and echocardiograms.
What about preventing endocarditis?
Talk with your child’s health care team about your child’s risk for endocarditis, an infection in the heart. Ask if antibiotics are needed before certain dental or medical procedures. Good oral care is important for everyone and can help lower the risk of infection.
d-Transposition of the great arteries in adults: What to expect
Babies born with d-TGA cannot survive for long without treatment or adequate mixing of blood. Surgery is needed early in life so they can live through childhood and into adulthood. Because of this, almost all adults with d-TGA had surgery as children. As adults, they may have health issues related to earlier surgery or to heart problems that could not be fully repaired.
How was my d-transposition repaired in childhood?
As a baby, you may have had a temporary procedure in a cardiac catheterization lab to help stabilize your heart before surgery. The procedure enlarged a natural opening between the right and left upper chambers (the atria). It allowed oxygen-rich blood to mix with oxygen-poor blood so more oxygen could reach the body. This opening was later closed during heart surgery.
There are two main types of surgery that have been used to repair d-TGA:
- Atrial switch surgery (Mustard or Senning procedure): The surgery was developed in the late 1950s and was commonly used in the past. It created a tunnel (called a baffle) inside the heart to reroute blood so oxygen-rich blood could reach the body and oxygen-poor blood could reach the lungs.
- Arterial switch operation: This is the surgery most commonly used today. The aorta and pulmonary arteries are moved to their normal positions. The aorta is connected to the left side of the heart, and the pulmonary artery is connected to the right side. The coronary arteries, which supply blood to the heart muscle, are carefully reattached.
Will more repairs need to be done in adulthood?
In most cases, people who had d-TGA repaired in childhood do not need another major repair. However, in rare cases, someone who had an atrial switch surgery may need more treatment. Doctors may evaluate if the heart can be changed to a different repair, using the arterial switch operation. This is a complex, staged process. Because the heart has been working in a different way for many years, the left ventricle may need special prep before this kind of surgery is done. This type of treatment carries risks and is offered only at highly specialized centers. It is usually considered only for carefully selected teens or young adults.
What problems might I still have?
Some adults who had the atrial switch surgery may develop heart-related problems over time. They can appear in young adulthood or after.
Because this surgery involved work inside the upper chambers of the heart, scar tissue may form. This can lead to abnormal heart rhythms. Also, with this type of repair, the right ventricle remains the heart’s main pumping chamber. Over time, it can become weaker and lead to symptoms of heart failure, such as fatigue or shortness of breath. Some patients will develop blockage in the tunnels, or baffles, that were created to redirect blood flow.
For people who had an arterial switch operation, the risk of long-term problems appears to be lower than with older surgeries. Early follow-up results have been encouraging. At the same time, this surgery has not been done for as many decades as atrial switch surgery. Possible issues include leaky heart valves or problems with the coronary arteries.
Ongoing Care
All adults with repaired d-TGA need regular care from a cardiologist who specializes in adults with congenital heart disease. Routine checkups may include noninvasive tests such as an electrocardiogram (EKG), echocardiogram, Holter monitor and stress test. Your cardiologist may also recommend other tests, such as a heart MRI or heart catheterization.
If you have a pacemaker, you will need more frequent visits. You should also see a cardiologist with expertise in caring for adults with congenital heart disease before any non-heart surgery or invasive medical procedure.
Medical treatment and follow-up
Some adults may need medications to help the heart work better. These medications can help the heart pump better, reduce fluid buildup and control blood pressure. Together, they can help manage symptoms of heart failure.
If the heart rate becomes too slow, a pacemaker may be needed. If the heart beats too fast or irregularly, medications may help control the rhythm. In some cases, doctors may ask for a catheter-based test and treatment called an electrophysiology study to better understand and treat heart rhythm problems.
For people who had an atrial switch surgery, blockages can sometimes develop in the tunnels, or baffles, that redirect blood flow. These blockages can often be treated with stents to help keep the blood moving freely.
Activity restrictions
Many people with repaired d-TGA can be physically active. In general, health care professionals encourage physical activity because it supports heart health, fitness and overall well-being. Talk with your cardiologist to discuss your goals and the right level of activity for you.
Preventing endocarditis
Talk with your health care team about your risk for endocarditis, an infection in the heart, before or after surgery. Ask if antibiotics are needed before certain dental or medical procedures. Good oral care is important for everyone and can help lower the risk of infection.
Pregnancy
Many women with repaired d-TGA may have successful pregnancies depending on their heart function and overall health. The risk from pregnancy to the mother increases if heart failure or arrhythmias exist. It's important to consult with a multidisciplinary team, including an OB/GYN and a cardiologist experienced in caring for patients with congenital heart defects, before pregnancy. It is also important for women with repaired d-TGA to be seen in centers with high-risk obstetrical services and adult congenital heart disease expertise.
Will I need more surgery?
People who had an atrial switch surgery may need catheter-based treatments or surgery to fix problems with the tunnels that redirect blood flow, repair heart valves or treat heart rhythm problems. Both slow and fast heart rhythms can occur, and some people may eventually need treatments such as medications, procedures or a pacemaker.
For people who had an arterial switch operation, the need for more surgery is less common. In some cases, more treatment may be needed to relieve narrowing in the arteries where surgery was done or to repair leaky valves.





